Obinoscopy:
CLINICAL PHARMACOLOGY OF RENAL DISEASE
The kidney is a very important organ in our body despite its small size. It helps with the removal of waste products and maintains homoestasis. The kidney filter the extracelluar fluid volume across the renal glomeruli an average of 12 times a day. The kidney has a very important role in blood pressure regulation (via the renin-angiotensin-aldosterone system RAAS), in red blood cell production (via the production of erythropoietin) and in bone formation/remodelling (via the hydroxylation of vitamin D to its active form: 1, 25 dihydro Vitamin D). This means that anyone with kidney issues might have lots of problems such as hypertension, osteoporosis, anemia, and diseases due to poor homoestasis (eg hyperphosphatemia, hyperkalemia, metabolic acidosis, vitamin D deficiency, etc). Also, some of the drugs we take need to be metabolised and/or excreted by the kidney, thus those drugs either need to be stopped or their dosing frequency or strength reduced else they could be toxic. As pharmacologists, we need to know these drugs. I will list some of them here.
There are two type of renal disease, the acute renal disease and the chronic renal disease. From the name, the difference between the two is the onset duration. For acute, it takes hours to days to develop while for chronic it takes months to years to develop. I will dwell more on the chronic form (generally called Chronic Kidney Disease or CKD for short) as it’s the most common and the most insidious.
Like I said earlier, CKD is a progressive loss of kidney function over a period of months or years. Approximately 30 million US adults (more than one in seven) have CKD – the risk is highest in African-Americans and other non-Caucasians. As usual, we don’t have any reliable data for Nigeria – which is sad as lots and lots of people have kidney issues in this country. An evidence to this fact is the number of celebrities that have kidney issues (OJB Jezreel, Muna Obiekwe, Biglo, Fred Ekata, Samuel Adesanya, Emma Ugolee, Leo Mezie, Prince James Uche, Gbenga Ajumoko). However, it is estimated that about 10% of the world’s population is affected by CKD. End Stage Renal Disease (ESRD) is the most advanced stage of CKD. At this stage, the only solution is either dialysis or kidney transplant else the patient will die.
The most common cause of CKD is diabetes. This is followed closely by hypertension. Also some drugs can cause kidney disease. These drugs are: Aminoglycosides, Amphotericin B, Cisplatin, Cyclosporine, Loop Diuretics, NSAIDs, Polymyxins, Radiographic Contrast Dyes, Tacrolimus, Vancomycin, etc. Of all these drugs, I’d say NSAIDs are the heavy culprit because of its accessibility and rampant use and misuse.
The functional unit of the kidney is the nephron. Each nephron comprises the glomerulus, the proximal and distal convoluted tubule, the descending and ascending loop of henle, and the collecting duct. Filtration occurs at the glomerulus while reabsorption occurs at the loop of henle and convoluted tubules. Substances with molecular weight < 40000 daltons (including most drugs) can pass through the glomerular capillaries, larger substances (protein and protein bound drugs) are filtered out. The protein albumin is ideally supposed to be filtered out at the glomerulus due to its large size. If the glomerulus is damaged however, some albumin passes into the urine (albuminuria). The amount of albumin in the urine is used along with the Glomerular Filtration Rate (GFR) to assess the severity of kidney disease. We also use Blood Urea Nitrogen (BUN) and Serum Creatinine (SCr) to assess severity of kidney disease. The Kidney Disease Improving Global Outcomes (KDIGO) guidelines recommend using GFR, degree of albuminuria and cause of CKD to determine the degree/stage of renal impairments (there are 5 stages). A GFR < 60ml/min/1.73m2 and/or albuminuria (albumin excretion rate AER ≥ 30) indicates that the patient has CKD and specific treatment is warranted to prevent progression of the disease.
Angiotensin Converting Enzyme Inhibitors (ACEIs) or Angiotensin Receptor Blockers (ARBs) are firstline drugs to prevent progression of disease in patients with CKD, diabetes or hypertension if albuminuria is present. Patients with stage 5 has kidney failure (ESRD) which requires either dialysis or transplant only.
During treatment, there is need to also address the possible complications of CKD such as osteoporosis, anemia, and diseases due to poor homoestasis (eg hyperphosphatemia, hyperkalemia, metabolic acidosis, vitamin D deficiency). Treatment mostly requires supplementation with the deficient substance (vitamin D – Calcitriol, Cinacalcet, erythropoietin – Epoetin Alfa, Darbepoetin Alfa, etc) and/or the use of binders to remove excesses (Phosphate Binders such as Aluminium Hydroxide, Calcium Acetate, Calcium Carbonate, Ferric Citrate, etc., Potassium Removers such as Furosemide, Sodium Polystyrene Sulfonate, Patiromer, Dialysis, etc.). Treatment of hyperkalemia actually involves 3 steps. Step one is the stabilizing the heart with Calcium Gluconate, step two is moving some of the potassium into the cells using Insulin + Dextrose, Sodium Bicarbonate and Albuterol, and step three is removing the remaining excess potassium out of the body using Diuretics or Potassium Removers. Metabolic acidosis is treated using Sodium Bicarbonate and Sodium Citrate/Citric Acid solution.
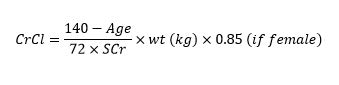
Certain drugs are contraindicated in CKD. This is primarily because those drugs are metabolised by the kidney thus they will accumulate in patients with CKD and elicit immense toxic effect. What we mostly use to determine if a drug is contraindicated or not is Creatinine Clearance (CrCl) which is calculated using the Cockcroft-Gault Equation. The equation is stated below:
https://s01.geekpic.net/di-AB335R.jpeg
Drugs like NItrofurantoin is contraindicated if CrCl < 60 ml/min, Voriconazole IV is contraindicated if CrCl < 50 ml/min, Tenofovir Disproxil Fumarate is contraindicated if < 50 ml/min, Tenofovir Alafenamide is contraindicated if < 30 ml/min. Other medications contraindicated when CrCl < 30 ml/min include NSAIDs, Dabigatran (when used for treatment of deep vein thrombosis and pulmonary embolism, DVT/PE), Rivaroxaban (when used for treatment of DVT/PE), Bisphosphonates, Duloxetine, Potassium Sparing Diuretics, Tramadol, etc. Note that Tenofovir has two different forms, the Disoproxil Fumarate form is affected more by CKD than the Alafenamide form. So we should be aware of the HIV brands that has either form. Brands that has the Disoproxil Fumarate form are Viread, Truvada, Atripla, Complera, Stribild while brands that has the Alafenamide form include Descovy, Bictarvy, Genvoya, etc.
Besides CrCl, we also use the estimated Glomerular Filtration Rate (eGFR) to estimate kidney function when dosing certain medications. The equation for eGFR is provided below:
https://s01.geekpic.net/di-09A5IN.jpeg
Drugs like Metformin, Sodium Glucose coTransporter 2 inhibitors (SGLT2i) , Meperidine, etc. are contraindicated if eGFR < 30ml/min/1.73m2
As can be seen from both formulas for CrCl and eGFR, they can be easily measured. All you need is the serum creatinine level, the rest (age, weight, sex, race) are pretty easy to measure. It is highly recommended that either CrCl or eGFR is measured for patients about to commence these medications.
There are drugs that are not contraindicated in CKD but rather require dosing modifications (ie reduction in dose). I will list some of them here: Fluconazole, Quinolones (except Moxifloxacin), Metoclopramide, Aminoglycosides, Beta-Lactam Antibiotics (except Anti-Staphylococcal Penicillins and Ceftriazone), Enoxaparins (Low Molecular Weight Heparins, LMWHs), Bisphosphonates, Lithium, Famotidine, Ranitidine, Rivaroxaban (when used for treatment of Atrial Fibrillation, AFib), Apixaban (when used for treatment of AFib), Dabigatran (when used for treatment of AFib), etc. For these drugs, we are to reduce the dose to prevent toxicity. Sometimes, the dose reduction can even get up to 40 – 50% or more. For Aminoglycosides, rather than reducing the dose in CKD, its preferable to increase the dosing interval (eg from tid to bid). Thankfully, there are drugs that are not metabolised by the kidney so we don’t have to worry about reducing their dose. It is preferable to give those drugs to patients with CKD. Some of those drugs include: Moxifloxacin, Anti-Staphylococcal Penicillins (Nafcillin, Oxacillin), Ceftriazone, Metoprolol, Carbamazepine, Zolpidem, Fentanyl, Levomethadone, Amiodarone, Pioglitazone, Gliclazide, Gliquidone, etc.
As I said earlier, if CKD progresses to failure (stage 5 disease), dialysis is required in all patients who do not receive a kidney transplant. The two primary type of dialysis are hemodialysis and peritoneal dialysis. In hemodialysis, we use a dialyzer while in peritoneal, we use the patient’s peritoneal membrane as the dialyzer. During peritoneal dialysis, the dialysis solution (usually containing glucose) is pumped into the peritoneal cavity. The solution is left in the abdomen to dwell for a period of time, then is drained. This cycle is repeated throughout the day, every day. When a patient receives dialysis, we must consider the amount of medication cleared during dialysis in order to recommend the correct dose and interval. Medications that are removed during dialysis (including many antibiotics) must be given after dialysis or may require a supplemental dose following dialysis. Drug removal during dialysis depends on the following factors:
1. molecular weight: smaller molecules are more readily removed by dialysis
2. volume of distribution (Vd): drugs with large Vd are less likely to be removed by dialysis
3. protein-binding: highly protein-bound drugs are less likely to be removed by dialysis
In conclusion, CKD is highly prevalent in Nigeria. Its progress is very insidious, thus there is need for us to actively monitor our patients renal function. This involves calculating a patients CrCl and/or eGFR and also ascertaining other comorbidities such as hypertension, diabetes, etc. As drug experts, we need to know drugs that are contraindicated in CKD as well as drugs that can cause or worsen CKD. We also need to know drugs whose metabolism depends on renal function as their dosage will be affected in patients with CKD. CKD treatment is multifactorial, it involves treating all possible comorbidities and signs/symptoms. Stage 5 CKD can also be treated using dialysis or kidney transplant.
REFERENCE
Brunton LL, et al. The Pharmacological Basis of Therapeutics, 13th edn. McGraw-Hill, 2018.
Hartmann B, et al. Drug Therapy in Patients with Chronic Renal Failure. Dtsch Arztebl Intl. 2010;107(37):647-656.
Katzung BG, et al. Basic Clinical Pharmacology, 14th edn. McGraw-Hill, 2018.
KDIGO CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Inter., Suppl. 2013;3:1-150.
Mula-Abed WS, et al. Estimated Glomerular Filtration Rate (GFR): A Serum Creatinine-Based Test for the Detection of Chronic Kidney Disease and its Impact on Clinical Practice. Oman Med J. 2012;27(2):108-113.
Zeind CS, Carvalho MG, et al. Applied Therapeutics: The Clinical Use of Drugs, 11th edn. Wolters Kluwer, 2018.
cc: Nairaland medical community impressive |








{kind=link}
{kind=link}