Akanke79's Posts
Nairaland Forum › Akanke79's Profile › Akanke79's Posts
1 2 3 4 5 6 7 8 ... 27 28 29 30 31 32 33 34 35 (of 44 pages)
This guy photographed every stage of his wife’s cancer treatment From Angelo Merendino’s blog: The first time I saw Jennifer I knew. I knew she was the one. I knew, just like my dad when he sang to his sisters in the winter of 1951 after meeting my mom for the first time, “I found her.” A month later Jen got a job in Manhattan and left Cleveland. I would go to the city – to see my brother, but really wanting to see Jen. At every visit my heart would scream at my brain, “tell her!!” but I couldn’t work up the courage to tell Jen that I couldn’t live without her. My heart finally prevailed and, like a schoolboy, I told Jen “I have a crush on you.” To the relief of my pounding heart, Jen’s beautiful eyes lit up and she said “Me too!” Six months later I packed up my belongings and flew to New York with an engagement ring burning a hole in my pocket. That night, at our favorite Italian restaurant, I got down on my knee and asked Jen to marry me. Less than a year later we were married in Central Park, surrounded by our family and friends. Later that night, we danced our first dance as husband and wife, serenaded by my dad and his accordion – ♫ “I’m in the mood for love…”♫ Five months later Jen was diagnosed with breast cancer. I remember the exact moment… Jen’s voice, and the numb feeling that enveloped me. That feeling has never left. I’ll also never forget how we looked into each other’s eyes and held each other’s hands. “We are together, we’ll be ok.” With each challenge we grew closer. Words became less important. One night Jen had just been admitted to the hospital, her pain was out of control. She grabbed my arm, her eyes watering, “You have to look in my eyes, that’s the only way I can handle this pain.” We loved each other with every bit of our souls. Jen taught me to love, to listen, to give and to believe in others and myself. I’ve never been as happy as I was during this time. Throughout our battle we were fortunate to have a strong support group but we still struggled to get people to understand our day-to-day life and the difficulties we faced. Jen was in chronic pain from the side effects of nearly 4 years of treatment and medications. At 39, Jen began to use a walker and was exhausted from being constantly aware of every bump and bruise. Hospital stays of 10-plus days were not uncommon. Frequent doctor visits led to battles with insurance companies. Fear, anxiety and worries were constant. Sadly, most people do not want to hear these realities and at certain points we felt our support fading away. Other cancer survivors share this loss. People assume that treatment makes you better, that things become OK, that life goes back to “normal.” However, there is no normal in cancer-land. Cancer survivors have to define a new sense of normal, often daily. And how can others understand what we had to live with everyday? My photographs show this daily life. They humanize the face of cancer, on the face of my wife. They show the challenge, difficulty, fear, sadness and loneliness that we faced, that Jennifer faced, as she battled this disease. Most important of all, they show our Love. These photographs do not define us, but they are us. Cancer is in the news daily, and maybe, through these photographs, the next time a cancer patient is asked how he or she is doing, along with listening, the answer will be met with more knowledge, empathy, deeper understanding, sincere caring and heartfelt concern. “Love every morsel of the people in your life.” – Jennifer Merendino These photos speak volumes. Brace yourself. https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/01-5dEsy7s.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/02-zC1A5tb.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/03-BiOWnec.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/04-V4LichX.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/05-EuzamVt.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/06-aXhNN2H.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/07-lQV4MQI.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/08-nhBJjeD.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/09-O5tz0Lf.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/10-wAzfI3m.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/11-T86Pc6I.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/12-3XSuqdU.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/13-bZckHye.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/14-EbHFRR9.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/15-c8n2d9d.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/16-ogZ90NU.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/17-YOMt8nY.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/18-ovItc24.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/19-tY0APdP.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/20-I2tE1Tk.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/21-GlBEPRY.jpg https://www.chrisbeatcancer.com/wp-content/uploads/2013/10/22-rZIpEuG.jpg All photos by Angelo Merendino. 3 Likes 1 Share |
As a part of NewsHour Connect, which showcases some of the best public broadcasting reporting from around the country, Enrique Cerna of KCTS in Seattle reports on the potential dangers of chemotherapy to caregivers who handle them. Lifesaving cancer drugs may put workers' lives at risk Chemo could have a hidden deadly toll on pharmacists, nurses By Carol Smith InvestigateWest updated 7/11/2010 Sue Crump braced as the chemo drugs dripped into her body. She knew treatment would be rough. She had seen its signature countless times in the ravaged bodies and hopeful faces of cancer patients in hospitals where she had spent 23 years mixing chemo as a pharmacist. Now she hoped those same medicines would kill the tumor cells lurking in her belly. At the same time, though, she wondered whether those same drugs may have caused her cancer to begin with. https://media4.s-nbcnews.com/j/MSNBC/Components/Photo/_new/g-hlth-100708-suecrump.grid-6x2.jpg Sue Crump prepares to receive chemotherapy for pancreatic cancer at Evergreen Hospital in Kirkland, Wash., before her death last September. Before her diagnosis, she spent 23 years mixing chemo as a hospital pharmacist and believes the years of toxic exposure caused her own cancer. Harnessing toxic agents to save a life demands a delicate balance. Chemo is poison, by design. Descended from deadly mustard gas first used against soldiers in World War I, now it’s deployed to stop the advance of cancer. Crump knew she had her own war on her hands. And she wanted young pharmacists and nurses to pay attention to her story. Little workplace regulation The same powerful chemotherapy drugs that have saved hundreds of thousands of patients’ lives for decades have at the same time potentially taken a deadly toll on the hospital and clinic workers who handled them. Crump, who died of pancreatic cancer last September at age 55, was one of thousands of health care workers who were chronically exposed to chemotherapy agents on the job for years before there were any safety guidelines in place. Now, some of those workers, like Crump, are being diagnosed with cancers that occupational health specialists say could be linked to that exposure. https://media2.s-nbcnews.com/j/MSNBC/Components/Photo/_new/100708-suecrump-hlg-2p.grid-6x2.jpg .Patty Allen, a long-time friend, holds Sue Crump's hand during a visit to say goodbye to her in hospice care in Kirkland, Wash. Their ranks include Bruce Harrison of St. Louis, Karen Lewis of Baltimore — both pharmacists —and Brett Cordes, a veterinarian from Scottsdale, Ariz. All, like Crump, worked extensively with or around chemotherapy. (See profiles below.) All of them eventually got cancer, or in Lewis’ case a pre-cancerous condition. All believed their disease was linked to workplace exposures and became symbols for increased safety. Cordes, who was diagnosed four years ago at age 35, and Lewis, who was diagnosed in her 50s, are both undergoing treatment. Harrison died at age 59. Tracing an individual’s cancer to a particular exposure is difficult. It’s one of the main reasons safety advocates have been thwarted in their efforts to get stricter regulations. But many who study these agents fear lax safety standards are resulting in ongoing exposures that continue to put current workers at future risk. A just-completed study from the U.S. Centers for Disease Control, 10 years in the making and the largest to date, confirms that chemo continues to contaminate the workspaces where it’s used, and in some cases is still being found in the urine of those who handle it, despite knowledge of safety precautions. "There is no other occupation population (that handles) so many known human carcinogens,” said Thomas Connor, a research biologist with the National Institute for Occupational Safety and Health. Connor has spent 40 years studying the effect of chemo agents on workers, and is one of the lead authors on the latest study. Chemo agents have been classified as “hazardous drugs” by the Occupational Safety and Health Association (OSHA.) Hazardous drugs are those known, or suspected to cause cancer, miscarriages, birth defects, or other serious health consequences. But an InvestigateWest investigation has found that OSHA does not regulate exposure to these toxic substances in the workplace, despite evidence of ongoing contamination and exposures. While Deputy Assistant Secretary of Labor for OSHA Jordan Barab said the agency “has been concerned about the potential for healthcare workers to be exposed to hazardous drugs for some time,” he conceded in written responses to questions from InvestigateWest that the agency does not have the resources to issue standards “covering every safety and health hazard facing workers.” “Although this is an important safety and health issue, OSHA has not considered a standard to specifically address hazardous drugs in the healthcare setting,” he wrote. OSHA has no regulatory authority to enforce safety practices with fines or sanctions, other than under its “General Duty” clause — a catch-all regulation that allows OSHA inspectors to warn an employer if they see something that concerns them. According to documents obtained by InvestigateWest through the Freedom of Information Act, OSHA has only used the clause once in 10 years to cite any health care institution, including hospitals, clinics, dental and veterinary offices, for their handling of hazardous drugs. Longterm exposures to ‘just a little bit’ A few months before she died, Crump sat in a coffee shop near her home in suburban Seattle, and perused a list of chemo drugs now deemed hazardous for health care workers to handle. She ran her fingers down the page. It’s a long list: cyclophosphamide, doxorubicin, fluorouracil, methotrexate. And the list went on. “Yeah, I worked with all of them,” she said. . Crump started at Seattle’s Swedish Medical Center in the early 1980s, before pharmacists used special protective “hoods” over countertops to contain spray and chemo contamination. They didn’t use gowns, or gloves. They had no reason to think they should. Occasionally, drugs would spill on the countertops. “We would wipe if off and throw (the towels) in the garbage,” Crump said. “Most of the chemo came in vials, and we would transfer it into plastic IV bags Sometimes there would be spray when they punctured the vials. Other drugs came in ampoules and would be squirted, she said. “I’d file the neck of it, then snap real fast, she said. “A lot of times, I got cuts http://www.nbcnews.com/id/38114586/ns/health-cancer/t/lifesaving-cancer-drugs-may-put-workers-lives-risk/#.VINoJlItDIU https://www.youtube.com/watch?v=nvldyOyv--0 https://www.youtube.com/watch?v=UgTYIswJ9i8 |
Cut Poison Burn Official Trailer https://www.youtube.com/watch?v=SCmr2OGmMDQ https://www.youtube.com/watch?v=YNKLSwmkSrU |
https://www.youtube.com/watch?v=V0WIN0gEEQA The people who are commonly referred to as “African Americans” in reality have no direct bloodline connection to the people on the continent called Africa. One of the reason’s America is in such turmoil is because the people who are the stewards of North America have turned their backs on their ancestral homeland, America. |
Sen Obanikoro Declaration for office of Governor of Lagos State https://www.youtube.com/watch?v=TyWhjJJeOmY&app=desktop |
In 1958, Dr Zubrod set about establishing an ambitious program to test over 30,000 species of North American plants for anticancer activity. The botanists charged with this collection job gathered up sack-fulls of twigs, needles, leaves and bark from thousands of different trees and bushes and sent them back to the NCI. Back in the NCI laboratories, crude extracts were made from these samples by dissolving the plant material in different solvents such as water or alcohol. These crude extracts, each containing thousands of individual chemicals, were tested for their ability to kill cancer cells growing in a test-tube. Where an extract proved to have anticancer activity, the enormous task of separating out the thousands of chemicals within each active extract then had to be undertaken in order to identify the active ingredient or ingredients. The number of man-hours involved in identifying and then purifying a single active extract runs into the hundreds of thousands. One of the trees sampled was the Pacific yew tree, a slow-growing, old-growth forest tree on the Pacific Northwest coast of the US, with a sack of twigs and bark and leaves arriving back at the NCI in 1963. The extract from the bark (but not the twigs or needles) caused considerable excitement when it was found to have significant anticancer activity in the test-tube, triggering a lengthy 4-year process to identify the active ingredient amongst the thousands of other chemicals within the bark. That active ingredient eventually was identified as taxol, destined to become one of the most commonly used anticancer drugs in the modern era. The discovery and identification of taxol took another 8 years of painstaking research, with its chemical structure finally being published in 1971. However, that was not the end of the challenge. The chemical structure proved so difficult to synthesise that early animal studies and subsequent clinical trials of the drug had to be conducted using naturally- extracted material, a cumbersome exercise that required chemists to isolate the drug from tonnes of bark being collected from forests in the US Northwest. Given that all the bark from a fully-grown Pacific yew tree only yielded 500 mg of drug (enough for about 5 doses), few Pacific yew trees were left across North America with their bark intact. Progress was only going to be made if the drug could be synthesised, but it was to be another 10 years before that problem was cracked. By the time the whole natural product program was abandoned by the NCI in 1981, over 114,000 plant extracts and 16,000 animal extracts had been screened for anti- cancer activity. Over that 20-year period involving tens of millions of man-hours of botanists who collected samples, chemists who conducted the extraction of samples, and biologists who tested the extracts in the laboratory, taxol was the only drug of any significance that they had to show for all that effort. Taxol (1992) went on to be commercialised by the drug company, Bristol-Myers Squibb, and to become a mainstay of chemotherapy for a range of cancers including ovarian and lung cancer. Since then, chemists have found that relatively minor alterations to its structure produces new drugs with increased and different activities. As a family of compounds, taxol and its new spinoffs are known as taxanes. They work in a similar way to taxol, but do it in a better or stronger or different way. The best known of these is docetaxol, a drug used to treat a range of cancers including prostate, breast and lung cancer While taxol might have been the NCI‟s only real success in its natural products program, the institute still played a key role through its collaborative efforts in the development of a number of other important anticancer of natural origin. Drug companies and private research institutes were active in this area as well, sending their promising samples off to the NCI to take advantage of their screening resources. Extracts from a deciduous tree (Camptotheca acuminata) found in Southern China were sent to the NCI and found to have promising anticancer activity in the test-tube. The active ingredient subsequently was identified in 1966 as camptothecin. In clinical studies, however, camptothecin proved to be a disappointingly weak anticancer agent, but subsequent changes to its chemical structure resulted in the development of the more powerful drugs, topotecan and irinotecan. Topotecan is used for small cell lung cancer and ovarian cancer, and irinotecan (1994) for colorectal cancer. Anther plant, the Madagascar periwinkle, similarly has provided an important family of anticancer drugs known as vinca alkaloids. The discovery of these drugs has its roots in herbal medicine, where extracts of the Madagascar periwinkle had been used for centuries in Madagascar for the treatment of diabetes and hypertension, and as a disinfectant. The sap of this plant was poisonous, and subsequent chemical analysis of the sap found that it contained a wide range of toxic chemicals known as alkaloids. Two of these alkaloids subsequently were identified as vincristine and vinblastine. The NCI played a key role in identifying the anticancer properties of vincristine, with the drug being approved in 1963 as a treatment for leukaemia. Two Canadian researchers subsequently identified the anticancer properties of vinblastine when it was given as a tea to animals and found to cause a profound fall in their white blood cell levels. These twodrugs were used initially to treat leukaemia and lymphoma as alternatives to mustine and aminopterin, although they are used far more widely now for solid cancers such as breast and lung cancers. The other significant anticancer agent to be discovered in this way is doxorubicin. This compound owes its existence to work in the 1950s by an Italian research company that had initiated a program to search for newly identified soil microbes that hopefully would have antibiotic or anticancer activity. A particular soil sample collected from the area surrounding the Castel del Monte, a 13th century Italian castle, provided a new strain of bacteria that produced a bright red pigment. Coincidentally, independent French and Italian scientists subsequently discovered that this compound showed good anticancer activity against a range of mouse tumors. In recognition of this joint discovery, the two teams named the compound daunorubicin, after Daunii, a pre-Roman tribe that occupied the area of Italy where the compound was isolated, and the French word for ruby, rubis, describing the drug‟s color. Clinical trials of daunorubicin began in the 1960s, leading to the drug being used to treat acute leukemia and lymphoma. The Italian scientists then discovered that minor changes to the structure of daunorubicin increased both the strength of the anticancer activity and the range of cancers that it affected, including a range of solid cancers. They named this new compound adriamycin after the Adriatic sea, the name then being changed to doxorubicin when the drug came to market in 1974. Doxorubicin now is one of the most widely used drugs in the treatment of cancer. 5. Combination chemotherapy Prior to the mid-1960s, the standard method of chemotherapy for any cancer involved the single use of available drugs. Treatment would start with one drug and then move onto a second drug when the first one either failed to work after several weeks of trying or when an initial response was followed by a return of the cancer. The development of drug resistance remains one of medicine‟s great challenges whether it is in the field of infection (eg. Golden Staph), or parasites (eg. malaria) or cancer. Faced with annihilation by drugs, organisms have a remarkable capacity to fight back by developing resistance to those drugs. Cancer cells share this biological capacity along with bacteria and parasites. Considerable experience already had been gained with this phenomenon in tuberculosis, where the general experience was that the successive use of different antibiotics usually led to the infection becoming resistant to all antibiotics. But when antibiotics with different mechanisms of action were given as a combination, the risk of resistance developing was much less likely to happen. In the mid-1960s it was decided to test this notion with cancer. One group reported on the treatment of children with acute lymphoblastic leukaemia (ALL) with a combination of four drugs – methotrexate, vincristine, 6-mercaptopurine and prednisone – with most patients showing long-term remission. Subsequent refinements of this multiple therapy approach have led to ALL becoming a largely curable disease. A couple of years later, a second group from the NCI extended this observation to solid cancers, showing that a combination of mustine, vincristine, procarbazine and prednisone could lead to long-term remission in Hodgkin‟s and non-Hodgkin‟s lymphomas. Combination therapy comprising two or more anticancer drugs has become the standard form of chemotherapy in use today 6. The platinums The platinum-based drugs are worthy of highlight since, along with the taxanes and doxorubicin, they are the most widely used anticancer drugs today. Their history also underlines the extent to which a mixture of serendipity and scientific curiosity can play in the discovery of major drugs, in the same way that penicillin was discovered. They also play a role in the phenoxodiol story and are worth looking at from that point alone. The platinum-based drugs are so-called because they are chemicals based around a central atom of platinum. They include cisplatin and its more recent derivatives, carboplatin and oxaliplatin. The origins of this drug date back to 1845, when a chemist by the name of Peyrone first showed that compounds could be made based around a platinum atom. There was little interest in this family of compounds until the 1960s when a researcher at Michigan State University made a fortuitous discovery. Barnett Rosenberg was interested in the effects of electricity on the growth of bacteria when he unexpectedly found that bacteria stopped dividing when placed in an electric field. This was an exciting observation, suggesting a potentially new form of sterilization. Believing that the effect was related to the action of the electric field per se, Rosenberg spent months trying to unravel the mechanism. To his disappointment, he ultimately found that the inhibitory effect was nothing more than an artifact, with the platinum electrode being used to generate the electric field undergoing electrolysis, producing platinum-based compounds that were inhibiting the ability of the bacteria to divide. This might have been a disappointing result for the future of sterilization, but it was a mightily important step in the future of chemotherapy. Fortunately for chemotherapy, Rosenberg had the foresight to see the potential of this accidental discovery, deciding to work with NCI to investigate the use of platinum- based compounds as potential nticancer agents. That led them back to the original work by Peyrone over a century earlier in terms of the chemistry required to create platinum-based compounds. One of these compounds, cisplatin (1978), proved to be a highly effective anticancer agent, subsequently becoming one of the most widely- used chemotherapies and revolutionizing the treatment of a wide range of common cancers. In particular, it provided an effective cure for testicular cancer. It took another two decades to understand how cisplatin was working, which was by binding to the DNA and physically preventing the DNA from dividing |
2. Second anticancer drug Mustine represented a promising start. Its effect on lymphoma was less than striking, but it did serve to prove that a cancer could respond to a toxic drug without jeopardising the life of the patient. What was required now was the development of drugs with more powerful actions. That step came just a few years later as a result of work coincidentally underway in Boston at Harvard Medical School. This work concerned the role of folic acid in cancer. As with mustine, the Boston work was not based on any particular understanding of cancer or the fact that damaging a cancer’s cell DNA was a good strategy to pursue for drug development. Instead, the work was based on an astute sense of logic along with a single-minded determination by a paediatric pathologist, Dr. Sidney Farber (1903-1973). The background to this work was a discovery a few years earlier in 1937 that a form of anaemia known as ‘tropical anaemia’ in children in Bombay (Mumbai), India, was correctable by supplementation with brewer’s yeast. The unknown factor in the yeast initially was called Wills factor, after Lucy Wills its discoverer, but subsequently identified as folic acid (or vitamin B9). These days we recognise that folic acid is an important nutrient because it is an essential building block of DNA and therefore is in high demand for rapidly growing cells, which is why nutritionists recommend folic acid supplementation for pregnant women and infants. But back in the 1940s, the connection between folic acid and DNA and cell growth had yet to be made. The extent of understanding about the role of folic acid in the body was based on the Wills work showing that folic acid corrected anaemia in children by stimulating the growth of bone marrow, the source of both red and white blood cells. Sydney Farber was attracted to this story because of his interest in the treatment of leukaemia. Farber worked at the Children’s Hospital in Boston which handled many cases of childhood leukaemia. At that time, this was a largely untreatable, painful disease that often led to death within weeks of diagnosis. Farber’s logic was simple – if folic acid stimulated healthy bone marrow to make red and white blood cells, then perhaps it also played a critical role in the excessive activity of bone marrow in producing white blood cells in leukaemia patients. He reasoned that by blocking the uptake of the cancer cells in bone marrow of folic acid, the production of leukaemic cancer cells might be slowed. Chemists at Lederle (now part of Wyeth) had successfully synthesized folic acid in 1945. In collaboration with Lederle, Farber had drugs designed that looked like folic acid, but which could not work like folic acid. The notion was that they would look sufficiently like folic acid to fool cells into taking them up, but once inside the cell would fail to provide whatever benefit the folic acid was thought to be providing. One of these drugs, aminopterin, proved very effective at doing this. When aminopterin was injected into the body, its levels in the body vastly exceeded the level of folic acid, leading to cancer cells taking it up to a much greater extent that folic acid. The rapidly dividing cancer cell with its high demand for folic acid needed to service its DNA expansion, suddenly found itself with non-functioning DNA because it contained aminopterin and not folic acid. In 1947, Farber treated a group of 16 children who were seriously ill with acute lymphoblastic leukemia with aminopterin and achieved remission in 10 patients, meaning that the clinical symptoms of the leukaemia disappeared. As with mustine in lymphoma patients, the remissions with aminopterin proved to be fairly short- lived, but again this was a key step in reinforcing the principle that aggressively- growing cancer cells could be successfully challenged by drugs. Farber published his findings in 1948 to curiously mixed reactions. The cancer research community, including his Harvard University colleagues, was largely dismissive. Part of this reaction appeared to be professional jealousy and had to do with a discovery of such magnitude being made by an unknown scientist working in a forgotten basement laboratory with little in the way of research funding. But there also was the accusation that leukemia was incurable and that affected children should be allowed to die in peace and dignity without needlessly suffering side-effects of chemotherapy. In the context of the day, where the idea that childhood leukaemias were curable by chemotherapy was unthinkable, such a view is perhaps understandable. And it has to be said that this is a debate that is as pertinent today as it was then, particularly in relation to the use of chemotherapy to extend life marginally in terminal cancer patients at the expense of quality of life. However, that point remains that Farber‟s work opened the door to research that ultimately shifted childhood leukaemias from a fatal disease to a largely curable disease. Interestingly, it was the non-research community, the doctors at the coal-face who were dealing with dying children, who gave Farber his greatest support and encouragement. Their eagerness to embrace anything that gave them an ability to alleviate suffering in children with leukaemia ensured that chemotherapy, at least for leukaemias, had a firm foundation. Aminopterin was replaced 5 years later by a more powerful version known as methotrexate (1953), and that drug remains a standard anticancer drug in use today. In 1958, methotrexate was shown to be an effective cure of choriocarcinoma, a rare cancer of the placenta in pregnant women. Despite its rarity, the significance of this discovery was that it was the first report of a solid cancer being cured by chemotherapy and was a critical step in establishing the concept of using chemotherapy to treat solid cancers as well as leukaemia where the cancer cells are single and unattached and not formed into a mass structure. 3. Co-coordinating the research effort As pivotal as the pioneering efforts of individuals such as Sidney Farber were to the establishment of the principle of chemotherapy, there is no doubt that it was the subsequent major injection of funds by governments and drug companies that ensured that chemotherapy expanded to meet its potential, and the one institution that stands out in this regard is the US National Cancer Institute. The extent of that impact is evidenced by the fact that by the mid-1990s, the NCI had played a role in the development of two-thirds of all anticancer drugs in use at that time. The NCI was created in 1937 by President Theodore Roosevelt as an independent research institute, and then brought under the umbrella of the National Institutes of Health based in Maryland in1944. One of the key contributions of the NCI has been to establish methodologies for screening potential anticancer compounds at a time when drug companies were beginning to show some interest in the development of anticancer drugs, but had little or no in-house facilities to evaluate their usefulness. The NCI eventually became a one-stop shop for cancer research, where it conducted its own basic research, provided a screening resource for other researchers, provided funding for other researchers, and coordinated the clinical testing of new anticancer drugs. It is a model that other countries had emulated to a greater or lesser degree, but the amount of funding that the NCI receives has ensured that it remains the pre- eminent cancer research institute that it always has been. 4. Drugs from Nature At the outset, scientists at the NCI and elsewhere adopted two main approaches to the discovery of anticancer drugs. The first was the approach taken by the Boston team in the development of aminopterin. This is known as rational drug design – meaning that you start with a known function (in this case the essential need for folic acid by the cancer cell), and you design a drug that deliberately interferes with that need. The other approach is more random…..to look for existing compounds within Nature. This approach doesn‟t require any understanding of how a potential drug might work, just the fact that it kills cancer cells. It is a needle-in-a-haystack approach that involves searching through the millions of species of plants, marine life, insects, coral etc for naturally-occurring chemicals with anticancer activity. Why would something like a plant or a coral or a microbe need to contain a compound capable of fighting cancer? Well, it doesn‟t….that is, these organisms don‟t succumb to any condition evenly remotely related to cancer, but most living things do need to make compounds that help them fight off predators such as a disease-causing organism, and one way to do that is to make the protective compound able to poison any threatening predator. Poisoning generally means that you disturb the invading-organisms biochemical processes to the point where it is dissuaded from attacking or perhaps is even lethal enough to kill it. And anything that is capable of causing that amount of harm to any living cell certainly has the potential to make a cancer cell sick. This looking-for-a-needle-in-a-haystack approach is a painstakingly tedious experience that is rarely rewarding. In fact it is more like looking for a needle in 10,000 haystacks. It usually means teams of people going out and collecting samples from jungles or forests or coral reefs, and then screening chemical extracts from hundreds of thousands of samples for some evidence of an ability to stop cancer cells from growing in the laboratory. And this is exactly the effort that the NCI embarked on in the 1950s. In 1956, Dr Gordon Zubrod was appointed head of the Division of Cancer Treatment in the NCI. Dr Zubrod formerly had been in charge of development of anti-malarial agents for the US Army and had a keen interest in natural product research, holding the not unreasonable view that Nature probably holds the keys to most of our ailments, particularly the degenerative diseases such as cancer, and that it is just a matter of investing enough time and effort to find those keys. |
1 Like |
The danger in this strategy lies with those parts of the body that have a high rate of cell turnover. Notably, the lining of the gut which is replaced every few days; red and white blood cells have a limited lifespan and need to be regenerated within the bone marrow of the long bones on a regular basis; and hair is being constantly produced within the hair follicles of the skin. This means that tissues such as these are going to be highly susceptible to the effects of DNA. The side-effects of gastro-intestinal toxicity are severe nausea, vomiting and diarrhoea. The side-effects of bone marrow toxicity are low levels of red blood cells, resulting in anaemia, and low levels of white blood cells, predisposing the patient to serious infections. The side-effect of hair follicle toxicity is baldness. These unwanted consequences on healthy tissue have exactly the same underlying mechanism of action as the burning symptoms seen in the eyes and lungs of World War 1 soldiers, and those seen in the citizenry of Bari. The use of cytotoxic anticancer drugs is based on the simple principle that the most rapidly dividing cells in a cancer patient’s body are the cancer cells, making them proportionally more likely to take up the drug than any other tissue. But tissues such as bone marrow and the gut inevitably will be hit by some collateral damage, making chemotherapy a delicate balance between poisoning as many cancer cells as possible while sparing as many healthy cells as possible – a delicate clinical dance between curing and harming. The side-effects of such chemotherapy also mean that there is a limitation to the number of times that the therapy can begiven or the length of time that it can be given. It is highly likely that chemotherapy with such anticancer drugs could effectively destroy most cancer cells in the body if they could be given in sufficiently high doses for enough time, but that would come at the cost of almost total destruction of the body. This delicate see-sawing between killing cancer cells and killing healthy cells also means that this approach is less likely to work with those cancers that are relatively slow-growing. Prostate cancer is an example of a slow-growing cancer. Chemotherapy with the kind of anticancer drugs that we are considering here is uncommonly used in early stage prostate cancer because the length of time that the treatment would need to be given as a function of the slow rate of turnover of the cancer would result in unacceptably high levels of side-effects. This delicate see-sawing between killing cancer cells and killing healthy cells also means that this approach is less likely to work with those cancers that are relatively slow-growing. Prostate cancer is an example of a slow-growing cancer. Chemotherapy with the kind of anticancer drugs that we are considering here is uncommonly used in early stage prostate cancer because the length of time that the treatment would need to be given as a function of the slow rate of turnover of the cancer would result in unacceptably high levels of side-effects. Anyway, back to our history. The mechanism by which mustine damages DNA is referred to as alkylation, a chemical term referring to the way in which the drug attached itself to the DNA, changing the DNA’s structure to the point where it could no longer function normally. In the 1950s, this discovery went on to spawn a family of anticancer drugs known as nitrogen mustard alkylating agents. Of these, the drugs chlorambucil (1957), melphalan (1957), cyclophosphamide, (1959) and streptozotocin (1982) are probably the best-known members of this family, and remain in wide use today for the treatment of cancers such as breast cancer, ovarian cancer, bladder cancer and chronic lymphocytic leukaemia. And despite its 60-year old age, mustine continues to be used occasionally today, mainly in a combined form with estrogen called estramustine, to treat prostate cancer. |
Up until just after the Second World War, there was no concept that drugs could be used to stop cancers growing. Surgery was essentially the only option, and then only reserved for the most easily removed tumours. Having an established, aggressive cancer at that time was in effect a death sentence. The first attempt at chemotherapy for cancer using scientific rationale was in 1946, and in one of the great ironies of medicine, owes its origins to war and to the notion of inflicting harm and misery on people. In the six decades since, the science of cancer chemotherapy has lurched ahead in fits and starts, with occasional periods of excitement and great promise breaking decade-long periods of little or no progress. The history of chemotherapy is marked by a number of key developments. 1. First patient, first anticancer drug Remarkably, the beginnings of chemotherapy are to be found in chemical warfare and a tragic, but ultimately fortuitous, war-time bungle. The story starts in the First World War with the development by Germany of nitrogen mustard gas that was used to such deadly effect in the trenches of Belgium and France. The gas was highly toxic, burning the skin, eyes and lungs of soldiers who inhaled it. Chemical warfare subsequently was banned by international treaty, so ensuring that the Second World War was essentially free of the use of toxic gases in the field. However, despite the treaty, both sides in the war were carrying out research into chemical warfare on a clandestine basis, with the US stockpiling nitrogen mustard gas in case Germany decided to use it as it had some 25 years earlier in France. In 1943, after the Allies had landed in Italy and were pushing up towards Germany, the US sent a supply of nitrogen mustard gas by ship to the Italian front, storing it in the Italian port of Bari. On the night of December 2, German bombers attacked the port, inflicting considerable damage including the warehouses holding the nitrogen mustard gas, releasing the gas across the city and exposing military personnel and civilians alike to the gas. Compounding the tragedy, neither military nor civilian physicians were informed about the presence of mustard gas in the city, leading to failure to properly treat hundreds of people affected by the gas. The extent of the damage associated with the release of the mustard gas is shrouded in controversy to this day, in part because of confusion over the proportion of casualties attributed directly to the bombing, and in part because of the highly classified nature of the event, with Churchill ordering that all records of the event be destroyed. Whatever the truth, it is uncontested that a considerable number of military personnel and civilians died as a result of exposure to mustard gas. The ongoing argument is over the extent of the casualties. Aware of the implications of what had happened, the US military sent pathologists to Bari to conduct autopsies on the casualties. The extent of what they found has never been disclosed, but one thing that they did find and did disclose is an unexpected finding of profoundly low levels of white blood cells in gas-affected bodies, with shrinkage of lymph nodes being particularly noted. Curiously, this effect had never been noted in the First World War despite the casualty rate from mustard gas poisoning running into the tens of thousands. This discovery so piqued the interest of the US Department of Defence that it recruited two pharmacologists, Drs. Goodman and Gilman, to look at the potential therapeutic applications of such an effect. Lymphoma, or cancer of lymph nodes, was an obvious target. The thinking was obvious – here is a cancer characterised by malignant swelling of lymph nodes, while on the other hand, nitrogen mustard gas was capable of shrinking lymph nodes in healthy people. The first step of the army pharmacologists was to come up with an injectable form of the gas that would allow a more defined dose to be delivered. To do this, they played around with the chemical structure of the nitrogen mustard molecule in order to convert it from a gaseous form to a liquid form. This sort of effort is the basis of organic chemistry – changing the structure of chemicals in the same way that oil molecules can be turned into molecules of petrol, or diesel, or kerosene, or plastics. One of the new structures that they settled on for further testing was the drug mustine. After confirming that mustine reduced lymphomas in mice, they then collaborated in 1945 with a thoracic surgeon, Dr. Linskog, to use mustine in a patient with non-Hodgkin’s lymphoma. The effect was dramatic, with the lymph nodes showing significant shrinkage. Unfortunately the response only lasted a few weeks, but the significance of this event was the promise of the principle that cancer could be treated by chemotherapy. At the time, there was no real understanding of how the drug was working. Here was a drug whose heritage was a capacity to inflict severe burns on the skin, eyes and lining of the lungs, and yet there was nothing particularly obvious at the time to link a burning effect to how it might be functioning as an anticancer agent. It would be another decade before it was discovered that mustine was working by attaching itself to the DNA of the cancer cell in a way that prevented the DNA from functioning normally. Just as the cancer had been caused in the first place by DNA damage, mustine was doing the same thing, only many times greater. The initial damage that led to cancer in the first place, by definition must have been relatively mild in order for the cell to survive and to evolve into a cancer cell. The amount of damage being inflicted on the DNA by mustine was so great that the cell had no option but to die. When used as a chemical warfare agent, the nitrogen mustard gas was inflicting lethal damage on the DNA of the cells lining the respiratory tract. In Dr Linskog‟s patient, it was doing the same thing, but concentrating its action on the lymphoma tumour. Ironically, although these early scientists were completely in the dark as to exactly how mustine was working, their discovery set the pattern for the way in which the vast majority of anticancer drugs would be developed over the next 60 years. The overarching principle that has guided the development of anticancer drugs has been that irreversible damage to a cancer cell’s DNA will put that cell’s ability to survive in jeopardy. Some drugs inflict so much damage on the DNA that the cancer cell simply cannot survive. These are known as cytotoxic drugs. These drugs usually result in almost immediate shrinkage or even complete disappearance of the cancer. Other drugs are less damaging, to the point where the cell is too damaged to divide but not so damaged that it will die. These drugs are known as cytostatic chemotherapies. The effect of these drugs is to stop the growth and spread of the cancer, without necessarily shrinking the cancer. The principal downside of this approach is that such drugs are by their very very nature non-selective. A drug that disrupts DNA function doesn’t distinguish between the DNA of a cancer cell and that of a normal, healthy cell. An anticancer drug once inside the body is perfectly able to penetrate any tissue in that body and to attach itself to any and all DNA, irrespective of whether it is healthy or cancerous DNA. The saving grace, the reason why most cytotoxic anticancer drugs can shrink cancers without shrinking our liver or heart to the same extent, is that the effect of the drug is dependant on the extent of DNA activity in the tissue. It is only when a cell is actively dividing that its DNA is at risk of damage from the drug. Cells that are sitting quietly, functioning normally but not dividing, are not at any particular risk of damage from the cytotoxic drug. That is the case for most of the major organs in our body. The rate of cell turnover in most parts of the body (such as the liver or heart) is so relatively low, that they are spared the worst effects of cytotoxic drugs. 1 Like 1 Share |
https://www.youtube.com/watch?v=xXyUf_cqHQ0 Dispatches challenges the claims made for the main anti-AIDS drug, AZT. In America later this evening, the results of a new study of life expectancy for those on the drug will be published. Those results will throw new doubts on the effectiveness of AZT. Tonight's Dispatch is the third on the subject of AIDS. As before, the programme's advice is clear; no-one should alter medication without consulting a doctor - still less, on the basis of a television programme. But the role of tonight's Dispatch is to examine the evidence. It will argue that in this country, the Wellcome Foundation, the manufacturers, are making false and misleading claims about the drug and could be in breach of the law. That's AZT - CAUSE FOR CONCERN. Meditel 1992 In May, 1990, the American AIDS activist group ACT UP organised a demonstration outside the National Institutes of Health in Maryland. They were protesting about AZT or zidovudine, the only approved drug for AIDS. This was a remarkable about turn because three years earlier other ACT UP demonstrations had clamoured for more AZT to made available at a cheaper price. What had changes? |
This is a video about an AFrican brother who got possessed by a chinese spirit when he went for acunpuncture for his hand,the jinn entered his muscle to make his hand feel good and continued to stay in his hand https://www.youtube.com/watch?v=40FaPJTPAmA |
Truck loads of Austria's popular Red Bull energy drink are being shipped daily by Turkish traders into Syria, and being consumed by fighters in the civil war who are drinking it to help them stay alert during gruelling battles. They are also making a profit from the cross-border business, generating money for more weapons, according to a report on Bloomberg. Trade statistics published in Ankara last week show that Turkey is shipping billions of dollars worth of goods into Syria. After President Bashar al-Assad’s government in Damascus lost control of most border crossings with Turkey rebel groups such as the Free Syrian Army and Islamic Front, as well as Islamic State extremists have been able to control trade. State control is absent and transporters pay tolls and fees to whoever controls the crossing. As well as practical things like vegetable oil and cement, traders are also taking amphetamines like Captagon across the border, but one of the most popular goods by far is Red Bull “Every day we have four or five trucks carrying Red Bulls to Syria,” Mustafa Yilmaz, owner of Turkish trucking company Cem-Ay Transport, said. Buyers on the Syrian side don’t identify themselves to the transporters, Yilmaz said. Goods are then transferred onto Syrian trucks in a three kilometre wide zone at the Cilvegozu crossing, he added. http://www.thelocal.at/20141110/red-bull-fuelling-syrian-islamists |
https://www.youtube.com/watch?v=QmqrFK4-OfQ While Christian Churches in the UK are struggling to draw people to worship, the Islamic community there is burgeoning. Some Muslim groups are doing all they can to counter fears the rapid growth is a challenge to British traditions. |
Racism whether upon open or hidden, is an evil aspect of life which Islams seeks to eradicate. It is clear from the versus of the Quran, and many sayings of the Prophet (saw) which have been narrated by his companions, that differences in colour, tribes, races, or traditions are not to be excuses for unjust behaviour or treatment. "O Mankind, we created you from a single pair of a male and a female, and made you in to tribes and nations so that you may know each other (not that you despise each other). Verily, the most honoured of you in the sight of Allah is he who is most righteous of you." (Al-Quran, Chapter 49, Verse 13) https://www.youtube.com/watch?v=3MqeSPF48tg |
This is a video about an AFrican brother who got possessed by a chinese jinn when he went for acunpuncture for his hand,the jinn entered his muscle to make his hand feel good and continued to stay in his hand https://www.youtube.com/watch?v=40FaPJTPAmA |
Watching inappropriate things and listening to music and its effect on shayateen (devils) The effect of listening to Qur'an on expelling shayateen and drawing in angels. We are not saying all media is haram, however, in all forms of media and entertainment there is that which Allah does not like the believers to see or listen to, due to its harmful effects on individuals and society. https://www.youtube.com/watch?v=CaULTYeGzD0 The importance of hijab in protecting believing women from the evils of the unseen world https://www.youtube.com/watch?v=eiG0H_p6fxc |
THE STORY OF ABU QUDAMA AND THE BOY This story will bring u in tears each and every time u listen Jazak allah khair By Brother Bilal Asaad https://www.youtube.com/watch?v=nAzRU07ULjM |
Strongly recommended, In shaa Allah all of you will be able to relate to it and benefit from it! https://www.youtube.com/watch?v=TgKBkbkjo34 |
I found this message on the net recommended by a brother. Assalamualaikum dear brothers and sisters, I am going to share with you my personal experience dealing with sihr and jinn. i have been a victim of sihr all my life. I have only found out about it 1 year ago but before that I had no idea about sihr/magic. I couldnt progress in life because of it, I have failed to get a proper education and job. I never get any marriage proposals. It also had a tremendous effect on my health and I have been suffering both mentally and physically all my life. I have seen a few raaqis since I found out about my sihr but let me tell you it is very difficult to find a good raaqi and I still have not managed to find a trustworthy raaqi. So, I am doing self ruqyah. It has been one year and a few months that I have started doing self ruqyah. I had my ups and downs during the process cause it is constant battle against the shaytan. I thank Allah for giving me the strength and support to fight this battle against my enemies. Although I am not yet completely cured from the sihr but I have improved a lot in many ways Alhamdulillah. Now I am going to share with you what I have been doing to beat the sihr but first let me tell you that there is no quick cure, so dont expect a quick recovery, you have to be very patient and work hard. This requires a lot of hard work. Things that you need to do 1. Put your complete trust in Allah only. Nobody but Allah can save you from this. Allah is the healer, the saviour. 2. Perfect your character. Control your speech from foul language, lying and backbiting and control your temper cause you rage and anger makes an easy access for the shaytaan. When you become angry, say Auzubillahiminash shaytanir rajeem 3 times or do wudu. 3. Be generous, spend in charity and always be ready to help people in need. 4. Say your prayers on time. Recite the fourth kalima 100 times at fajr time. Recite the morning and evening adkhaars everyday after fajr and asr prayer. You can find the morning and evening athkhaars in hisnul muslim. 5. Dont listen to songs or music. Remove all types of pictures from your house. Angels dont enter a house where there are pictures. 6. Play surah Baqarah loud in your house everyday. This has really helped me to remove the external jinns from my house Alhamdulillah. 7. Recite this ruqyah after every prayer. Start with durood shareef 11x, then recite Surah Fatiha 1x, Surah Baqarah verse 1-5 (1x), Surah Baqarah verse 255 (1x), Surah An Nisa verse 56 (3x), Surah Al Araf verse 117 -122 (1x) but verse 118 (3x), Surah Yunus verse 79-82 (1x) innlaha sa yubtiluhu (3x), Surah Taha verse 65-70 (1x) but the verse 69 to be recited 3x, Surah Yasin verse 1-12, Surah As-Saffat verse 1-10 (1x) but recite the verse 8 (3x), Surah Ad-Dukhan verse 10-18 (1x) verse 11 to be recited 3x, Surah Ad-Dukhan verse 43-48 (3x), Surah Al Ahqaf verse 29-32 (1x) recite verse 31 (3x), Surah Ikhlaas (1x), Surah Falaq (1x), Surah Naas (1x) then join together both of your palms and blow on your palms and wipe your palms all over your body, head and legs. End with durood shareef 11x. 8. Mix a tablespoon of blackseed oil in a big bottle of olive oil and recite this ruqyah into the oil mixture. Surah Fatiha 3x, Surah Baqarah verse 255 (3x), the last 2 verses of Surah Baqarah 3x, Surah Al Araf verse 117 -122 (3x), Surah Yunus verse 79-82 (3x), Surah Taha verse 65-70 (3x), Surah Ikhlaas 3x, Surah Falaq 3x and Surah Naas 3x. Recite durood shareef 11x before and after the ruqyah. Use this oil mixture from head to toe. you can also mix a few drops of musk into the oil for a sweet smell cause this might irritate the jinn even more. 9. Recite the same ruqyah from number 8 into a jar of blackseed honey and keep stirring the blackseed honey with your finger or with a spoon while your reciting the ruqyah in it. Drink a teaspoon of this honey every morning and evening. 10. Now prepare for ruqyah bath. Recite the same ruqyah from number 8 for the ruqyah bath. There are a few different ways to make the Ruqya bath but they are near enough the same. You will need the following listed ingredient for the bath. Ingredients: Saffron – 3 pinches Sidr (lote tree) leaves. 7 leaves, or 7 pinches if you have it in powder form 3 table spoons of Apple cider vinegar Dead sea salt (coarse, not powdered) Rosewater 1 litre of Water You can get most of these ingredients from a ‘middle eastern’ or ‘ethnic foods’ store. The Sidr leaves can be a little tricky, as in you cant always find them on the high street so you’re best bet is to try an Islamic book shop or ‘middle eastern’ store. Method All of the ingredients that you have should be recited upon or ‘blessed’. You can either recite upon the ingredients individually in their own bottles or you can put the ingredients into a bowl and recite upon the mixed ingredients. It’s better if you can recite upon them each time when you have put the ingredients into the bowl as the recitation is more effective [1] Put all of the ingredients into a bowl and recite the same ruqyah from number 8. Blow into the bowl – if you’re able to, it’s good if you can get some spittle into the bowl when you blow, try it by ‘wettening’ your lips with your salivah. Otherwise, just blowing onto it will suffice Take a small amount of Apple cider vinegar and massage it into your head, enough to cover your scalp/hair. Fill up your bath with warm water from the tap as you would if you were having a normal bath. Pour the contents of the bowl/ingredients into the bath. Sit in the bath for 30 minutes and submerge yourself as much as you can in the water. After some time, 10/20 minutes, Take the bowl and pour the water over your head at least three times or as much as possible. This will wash out the cider vinegar from your hair. After the bath, pat yourself dry but do not have a shower or wash off with soap afterwards – just pat yourself dry and leave it over night. You can have a shower in the morning inshaAllah. This is the best and most effective method. If you have followed these instructions you will see a difference inshaAllah. This is a very effective ruqyah bath and it has really helped me to get rid of some sihr Alhamdulillah. Do this bath everyday or every other day. 11. Now prepare recited water to drink. Recite Surah Fatiha 41x and Surah Yasin 1x, Surah Ikhlaas 3x, Surah Falaq 3x and Surah Naas 3x into a 2 litr bottle of water. This is called verses of healing. Dont forget to recite durood shareef before and after the surahs. Drink this water everyday. 12. Recite surah Yasin and Surah jinn everyday. 13. Pray salatul tahajjud (the night prayer) atleast 2-3 times a week. The more you pray, the better because this is a very beneficial prayer when duas are ready to be accepted. 14. Keep making dua and cry to Allah until healing occurs. Be strong and patient. Never give up hope on Allah. Remember you will get whispers from shaytan that the ruqyah is not working but dont stop doing ruqyah. You shouldnt give up. Be regular with your ruqyah baths, oils and other remedies mentioned. 15. Last but not least I forgot to mention a very important treatment for sihr, Hijama. Get Hijama done every month as this is extremely effective to beat sihr. I should mention that you will get some side effects during this process, like you might get body pain, vomiting, tightness in your chest, heartbeat, stomach cramps. Listen to Surah Baqarah when you see these symptoms. When I got body pain I massage my body with a massager while listening to surah baqarah. It really helped to ease my pain Alhamdulillah. If you have movements in your stomach or bloatedness then purchase senna leaves and make tea with them and drink every day for two weeks. I know this may look too much hard work but as I said it requires a lot of hardwork and theres no quick cure. Trust me, when you put your complete trust in Allah, everything becomes easy. Remember Allah is testing through this trial because you are beloved to Him. So, dont be sad and never give up hope. I pray that Allah grants you complete shifaa. Ameen. 2 Likes |
Q. Based upon your communication with possessing jinn, what are the main reasons why jinn possess humans? A. The reasons are as follows: 1. Walking around the house naked. 2. Being isolated and unprotected by the prophetic morning and evening prayers. 3. Entering the toilet without the fortifying prayers because the toilets are among the dwelling places of the jinn. 4. Pouring hot water on the jinn without mentioning Allaah’s name. 5. Going without making the fortifying prayers to areas of the jinn, like mountain tops and garbage dumps, hurting them by urinating on them or stepping on them – The jinn may then ignorantly hurt the person much more than he deserves. In such cases, the treatment involves addressing the jinn and telling it that the patient had accidentally – and not intentionally – hurt it. If it was harmed in the patient’s home, it should be told that it had not right to be there in the first place, for jinn are not allowed to live in the homes of humans. Thus, the jinn should be told that it is in the wrong. The will actually reply. Sometimes they will say, “I love him.” Other times they may threaten those in their presence by saying, “I will leave and hurt him.” In such cases, the exorcist must have strong faith and believe in the oneness of Allaah and say to the jinn, “You are certainly not able to do anything at all because the only one who can benefit or harm is Allaah.” At that point, the jinn will become fearful and cause the person to shake. Q. Who are most affected by jinn, men or women? A. Women are most affected because the jinn love beautiful women. They may even have intercourse with them. A case of possession was presented to me in which a Christian woman said that she feels something come upon her and she struggles with it but it overcomes her. I told her, “Accept Islaam and I will – by the grace of Allaah – remove it from you.” She refused, so I left her. Consentual intercourse can take place between them, but this would be a major sin because Allaah has created that which is suitable for each species. Thus, it is not allowable for humans to marry from the animal world. http://www.jinndemons.com/interview-with-mustlim-exorcist-sheikh-muhammad-taahir-about-jinn-possession/ |
Q. Based upon your communication with possessing jinn, what are the main reasons why jinn possess humans? A. The reasons are as follows: 1. Walking around the house naked. 2. Being isolated and unprotected by the prophetic morning and evening prayers. 3. Entering the toilet without the fortifying prayers because the toilets are among the dwelling places of the jinn. 4. Pouring hot water on the jinn without mentioning Allaah’s name. 5. Going without making the fortifying prayers to areas of the jinn, like mountain tops and garbage dumps, hurting them by urinating on them or stepping on them – The jinn may then ignorantly hurt the person much more than he deserves. In such cases, the treatment involves addressing the jinn and telling it that the patient had accidentally – and not intentionally – hurt it. If it was harmed in the patient’s home, it should be told that it had not right to be there in the first place, for jinn are not allowed to live in the homes of humans. Thus, the jinn should be told that it is in the wrong. The will actually reply. Sometimes they will say, “I love him.” Other times they may threaten those in their presence by saying, “I will leave and hurt him.” In such cases, the exorcist must have strong faith and believe in the oneness of Allaah and say to the jinn, “You are certainly not able to do anything at all because the only one who can benefit or harm is Allaah.” At that point, the jinn will become fearful and cause the person to shake. http://www.jinndemons.com/interview-with-mustlim-exorcist-sheikh-muhammad-taahir-about-jinn-possession/ |
“Each [person] has a succession of angels in front of him and behind him, protecting him by Allaah’s command.”[13] “He is the Irresistible, high above His servants, and He sends protectors over you…”[14] Whenever Allaah sees His servants being sincere and in constant worship, working in the service of mankind and Islaam, He protects the servant from the evil jinn by sending angels to protect him. I thank Allaah for protecting me and all who work in this field. Q. You mentioned earlier that your first session with a patient is an examination. If it leads to the conclusion that the patient is possessed, what is your next step? A. I begin the treatment sessions (jalasaat al-‘ilaaj). These sittings vary in length and number depending upon the case involved. The first of these sessions I call “purification of the heart” (“tat-heer al-qalb”). The idea being that the faith of the person whom I am to treat must be clear and pure. There should not be in his faith any paganism, evil, disbelief, hypocrisy or falsity. I therefore clean the heart first so that when the verses of treatment are read, they meet a pure heart. Otherwise, the verses will meet a defiled, sick heart not capable of treatment. This is comparable to planting a seed in infertile ground. It will not grow, but not due to any defect in the seed. The ground was not prepared for cultivation. The Third sitting I have named “purification of the psyche” (“tazkiyah an-nafs”), for Allaah has created man with a heart, mind, spirit/soul (rooh), psyche and a body. The treatments are aimed at the first four elements. The soul (nafs) is a combination of cravings (shahwah), instincts (ghareezah), emotions (‘aatifah) and inclinations (naz‘ah). So, we purify the sick patient’s psyche. If he smokes, drinks, gambles, lusts after women or is corrupt in any way, we purify it so that the psyche can help the heart. I also try to purify the psyche of other sicknesses, like anger, hatred, malice, jealousy, conceit, pride, arrogance, intemperance, greed and stinginess. This session is no less important than the second, for it is by the way of the evil psyche that the possessing jinnee establishes itself. Consequently, this level of treatment may require two, three or four sittings until the psyche of the patient is purified and contented. After this treatment, the psyche does not whisper to itself and it will block the whisperings of the devils. The fourth sitting concentrates on the mind, and I refer to it as “cleaning the mind” (“tanqiyah al-‘aql”). In this session I address how a person spends much of his time. If he reads useless materials, like love stories, pornographic materials, detective stories and newspaper articles, it only increase his remoteness from Allaah. I advise those who read such materials to give them up and replace them with reading the Qur’aan and its exegesis, authentic books of hadeeth, and books of law. I also encourage them to read useful books in other fields, like mathematics, philosophy, physics, engineering, etc. The final treatment can be one session or as many as six to twelve sessions. I call it “removing the spirit” (“takhlees ar-rooh”). It consists of removing the evil spirit from its hold on the human spirit. This is in accordance with a hadeeth recorded in the Musnad of Ahmad in which a companion of the Prophet () passed by a mad person and recited over him a legal ruqyah for six days, morning and evening.[15] Also in the hadeeth of Aboo Sa‘eed al-Khudree, Ibn Mas‘ood and others, it is recorded that the legal ruqyah should be repeated twice per day for six days. If it produces results, fine. If it does not, it means that something is incomplete from the previous steps. Therefore, I go back over all of the sessions and check the state of the patient. These sessions are followed by the prescription of precautionary measures (tahaffuzaat). When a patient gets well, doctors usually advise him to avoid certain foods in order to prevent the reoccurrence of the sickness. I do the same. I advise the patient to give up watching TV – especially the useless programs, to be consistent in performing his daily acts of worship, to get up at night for voluntary prayer, to read certain Qur’ânic verses daily, to repeat the declaration of faith a hundred times daily, to seek forgiveness from Allaah, to pray for the Prophet (). |
Location: Cairo Date: 9/8/88 Name: ‘Abdul-Khaaliq al-‘Attaar Date of Birth: 1920 Place of Birth: Cairo Education: Law degree from Cairo University, 1950. Memorized complete Qur’aan and studied sharee‘ah at the College of Law. Q. When and why did you begin to practice exorcism? A. About forty years ago one of my sons was afflicted by the jinn – although I did not know it at the time – and his sickness became a major problem for me. I went to many psychiatrists, psychologists, neurologists, brain specialists and a variety of medical doctors for treatment. But after every visit to the medical specialists his sickness became worse. Around that time, I happened to be reading Ibn Qayyim al-Jawziyyah’s book, Zaad al-Ma‘aad. In a chapter on the treatment of the possessed, I noticed that the symptoms of the possessed were the same as those shown by my son. The prescribed treatment mentioned in the chapter was the recitation of some Qur’ânic verses and prophetic supplications. So I recited over my son and he began to get better. His condition improved the more I recited until he became completely well – by the permission of Allaah. From that moment I felt a great desire to increase my knowledge of this science. Day and night I began to research the topic of the world of jinn, the devils and the angels. I read many books and many terrible ones. However – by the grace of Allaah – whenever I came across new information, I would not adopt it until after I had checked its authenticity based upon the Qur’aan and the Sunnah. What was confirmed, I accepted and what was not, I rejected. The correct information I recorded in my own notebooks until I had gathered many such notebooks and a large quantity of material. I then read extensively the writings of Imaam Ibn Taymeeyah (may Allaah be pleased with him) and his student Imaam Ibn al-Qayyim. Then I began to organize the information in chapters which lead – by the mercy of Allaah – to my writing of 30 books in the form of manuscripts about Qur’ânic medicine (at-Tibb al-Qur’aanee) and prophetic medicine (at-Tibb an-Nabawee). These books are ready for publication; however, due to my limited resources, I have been unable to publish any of them to date. Q. What percentage of the cases you meet are actual cases of demonic possession? A. When I visit someone or someone is brought to me who believes that he is affected by magic, evil eye, or the jinn, my first session is an examination (fahs) and giving advice. The method of examination is quite simple. Anyone afflicted by magic, evil eye or jinn attack must show some symptoms of the affliction, which I call, “symptoms of satanic bonding.” The symptoms have peculiarities like the symptoms of any other sickness, such as influenza and rheumatism. During the examination I, therefore, ask about the symptoms which may appear in both the walking state as well as during sleep. Symptoms during sleep include nightmares, sleeplessness, broken sleep, uneasiness, the grinding of teeth, and dreams of Satan in the form of carnivorous animals. Then I ask about symptoms while awake, such as feelings of anxiety, forgetfulness, hopelessness, lethargy and immobility. Included among the signs are being easily angered, crying, and staring aimlessly or avoiding eyes of others. If the patient displays such symptoms during his walking and sleeping states, I recite upon him some Qur’ânic verses. If he is possessed, the jinnee may begin at this point to talk either with the voice of the person or another voice. Sometimes it will use foul language, curse those present or strike and kick. It may reveal why it possessed the person and when it did so. It may also reveal if there are others present. Psychiatrists diagnose this as schizophrenia or dual personality. If a jinnee speaks through a human telling its name, religion and condition, they call it dual personality. If a jinnee does not speak but the person’s personality goes through a major change, they call it schizophrenia. Q. Are there other signs, like bad smells or an unnatural smile, that are common to possessed? A. In reality, when a jinnee bonds with a human, there are innumerable signs. Among them are laughter and crying for no reason. These symptoms were well-known to the medical profession and are explained as a result of overactivity or underactivity of certain glands. We know in spiritual medicine that this is due to demons playing with the glands, causing them to over-secrete or to decrease their secretions, therefore causing sudden changes in personality and swift mood shifts. The possessed person may also exhibit supernatural strength. Q. What is the percentage of real cases of possession among your patients? A. My shaykh and mentor, Imaam Ibn Taymeeyah (may Allaah have mercy upon him), who died more than 700 years ago, said in al-Fataawaaa the following, excellent statement, “If the veil were removed from the people of this time (Ibn Taymeeyah’s time, over 700 years ago), we would find most of the people of this time are possessed by demons.” If that was the case 700 years ago, what can we say about this age in which filth is widespread and the means of demonic possession are abundant. This is a time of sport and play, disobedience and corruption. The percentage of those possessed is very startling – may Allaah protect us all. Those spared demonic influence are very few, while those under attack are many. Allaah, the Almighty said in Soorah an-Nisaa’: “…rebellious devil, cursed by Allaah, said, ‘I will surely take a definite portion of Your servants and mislead them. I will create in them false desires and order them to slit the ears of cattle and to deface the creation of Allaah….’”[1] They are many. And Almighty Allaah’s statement: “And Satan proved his idea to be true on them, and they all followed him except a group of those who believed.”[2] So in reality, the percentage of those under satanic influence in the world today is extremely high. And there is a need everywhere for thousands and thousands of exorcists in order to help mankind achieve bliss in this life. There are a number of real sickness which the medical profession, past and present, in the East and in the West, has been unable to cure, and the cure lies only in the Noble Qur’aan. The medical profession readily admits it has not advanced over the years in its ability to cure problems such as epilepsy, bewitchment, and schizophrenia. In reality, those touched by Satan are so many and their percentage is rapidly increasing. Yet, those involved in treating them according to the Qur’aan and the Sunnah are so few that one cannot but fear for the future of mankind if a solution is not found. By Allaah’s blessing, I am working on passing on knowledge of this science to many young people. But resources to do this effectively are very limited. Q. From your own experience, what are the main reasons why people are possessed? A. I have written a chapter in my book, Iqtiraan ash-Shaytaan bi al-Insaan,[3] specifically for this question. There are exactly six reasons: 1) extreme fear, 2) extreme anger, 3) extreme jealousy, 4) devotion to lust, 5) human aggression against devils, and 6) love of demons for humans. Human aggression could be in the form of pouring hot water on the places where devils reside or urinating in holes or cracks in the ground. The Prophet () prohibited us from urinating in holes and cracks in the earth because they are places where the jinn reside. The love of demons for humans is very, very common. When male jinn possess human females and we communicate with them, they often readily admit that they are in love with them. And when female jinn possess men, they often express the same. Q. What is the percentage of females among your patients? A. They are about 70 percent of the cases. The percentage of possession among women is greater then it is among men. And this percentage is consistent with the texts of the Qur’aan and the Sunnah. On one occasion, the Prophet () visited a group of women and said, “Give in charity, because I was shown that you made up most of the inhabitants of the Fire.” When he was asked why, he replied, “You deny the good your husbands do whenever he makes a single mistake.”[4] Q. You mentioned about male jinn possessing human females and female jinn possessing men. Is this always the case? A. No. Sometimes female jinn possess human females and male jinn possess men. But I am unable to give you percentage as I did not keep a record of this. Q. When jinn speak through humans, do they use the same voice of the possessed? If not, what is the percentage? A. The Prophet () used to seek refuge in Allaah from what appears at night and is hidden during the day, and what is hidden at night and appears during the day.[5] And he also used to seek refuge in Allaah from every [evil] which announces itself and every [evil] which hides.[6] That which appears at night is that which speaks and that which is hidden is that which does not. Thus, speaking or not speaking of a jinnee through the voice of possessed is found in the Sunnah of the Prophet (). Even in the cases when the Prophet () treated those possessed, the jinnee did not speak with him or respond to him. The Prophet () struck the possessed person and said, “Get out, O enemy of Allaah, for I am the Messenger of Allaah!” And the jinnee did not reply to the Prophet (). But, in the case of the jinnee who was searching food and was caught by Aboo Hurayrah, it spoke with him. Also, the jinnee who possessed ‘Abdullaah ibn Mas‘ood communicated with him. Likewise, the jinnee who was beaten by ‘Umar bin al-Khattaab spoke with him. Another example is the female jinnee who spoke to Imaam Ibn Taymeeyah in the presence of his student, Ibn al-Qayyim, saying, “I love him.” And Shaykh al-Islaam Ibn Taymeeyah replied, “But he does not love you.” It then said, “I want to make hajj with him.” And Ibn Taymeeyah replied, “But he does not want to make hajj with you.” It said, “Then I will leave him for your sake.” Ibn Taymeeyah said, “No. Leave him in obedience to Allaah’s command.” This incident can be found in Ibn al-Qayyim’s book Zaad al-Ma‘aad in the chapter on prophetic guidance for treating the possessed. Likewise during the reign of the ‘Abbaasee caliph, Mutawakkil, the caliph informed Imaam Ahmad ibn Hanbal that one of his slave girls was possessed. Imaam Ahmad sent one of his students with a pair of wooden slippers and told him to tell the jinnee. “It is not permissible for you to inhabit this woman’s body, and Ahmad commands you to leave this woman’s body.” Al-Mutawwakil and others present heard the woman speak in a gruff, male voice, saying, “Ahmad’s command is welcome. For Ahmad is one who has obeyed Allaah, and Allaah has made everything obedient to him. If Ahmad ordered us to leave ‘Iraaq, we would leave.” Today, in many cases the jinn do speak, but in many other cases they do not. Q. Is possession a swift process or does it take a long time, like months or years? A. Medical doctors say that epilepsy is a sudden, unknown change in the electrical discharges of the brain. They say that there are more than 40 million electric discharges of the brain, and it is like a small electrical generating station. It produces electricity and distributes it throughout the other parts of the body. According to doctors, an epileptic fit occurs when there is a sudden surge in the electrical discharge of the brain. This overloads the circuit and leads to dysfunction in the body parts and becomes manifest in shaking, stiffness in the body parts, drooling and foaming at the mouth and staring lasting for a few brief moments. When we see such conditions, we call the adhaan in the epileptic’s right ear and call the iqaamah in the left ear and – by Allaah’s will – he becomes cured and returns to his normal state. Although the medical profession, ancient and modern, does not know the cause of the sudden increase in the electrical discharges of the brain, the Prophet () indicated a cause. In a hadeeth reported by Ibn ‘Abbaas (may Allaah be pleased with him), a black woman came to the Prophet () and said, “O Messenger of Allaah, I am overcome with fits and take off my clothes.” [and in another narration, “Verily, the evil jinnee takes off my clothes.”][7] In this hadeeth the Prophet () confirmed that it is the devil who causes people to fall down in fits. It has been demonstrated that the cause is demonic from the many cases in which we have called the adhaan in the ears of those in epileptic fits, and consequently the fits ceased. For the Prophet () has stated, “When Satan hears the adhaan, he turns and flees.” This is in the case of complete possession (sara‘ kullee). There are other types of possession in which humans are affected, like migraine headaches (sudaa‘ nisfee), insomnia (araq), depression, introversion (intiwaa) or pains occurring in different parts of the body at various times. The possessing demon who inhabits the human brain is able to vary cerebral electric discharges – by the will of Allaah – and affect the body parts with a variety of ailments. For example, it may affect the man’s tongue so that he cannot speak, his ears so that he cannot hear, his eyes so that he cannot see, or his hands so they tremble and become paralyzed. These are all various types of possession. Q. Have you experienced the jinn speaking in languages other than that of the possessed person? A. I have found many cases in which the jinn speak in other languages or other dialects common to other regions of the country. Q. Do the jinn enter the human body from particular points, like the mouth, eyes or hand? A. There are three types of jinn. One type consists of animals, such as dogs, snakes, donkeys and mules. These give birth to offspring like themselves. A dog-jinnee give birth to a dog-jinnee and a snake-jinnee gives birth to a snake-jinnee. Another type flies in the air, like the one mentioned in Soorah an-Naml: “And ‘ifreet among the jinn said, ‘I will bring it to you before you can rise from your position, for surely I am strong and trustworthy for that purpose.’ ”[8] I consider this type of jinnee like the TV picture which is transferred through the air. The jinn which enters the bodies of humans are from this type. Allaah referred to them at the beginning of Soorah al-A‘raaf: “Surely, he and his tribe see you from a position where you cannot see them…”[9] This verse means that the jinn see us, but we cannot see them. Air is with us everywhere. We sense it and are certain about its existence, but we cannot see it. The jinn are just like air, which is the meaning of Almighty Allaah’s statement in Soorah ar-Rahmaan: “And He created the jinn from a flame (maarij) of fire.”[10] Maarij is the hot air which is above the fire. Thus, the jinnee which enters the human body is not of the type which has a material form, like that of a human, donkey or dog. This type has a fine, invisible, ethereal (hawaa’ee) body. And it enters the body just like air does through the open orifices, like the mouth, the nose and the anus. Even the pores of the skin allow air to enter and thus become ports of entrance for the jinn. If we drink water in the summer, the water spreads throughout the body and passes out through the pores in the skin. Air also enters and along with it the jinn of this kind. However, the jinn usually live in the toilet areas use for defecation, urination and bathing. This is based upon the Prophet’s statement, “Surely, these hushoosh are inhabited.”[11] The hushoosh are the places used by humans to relieve and clean themselves. Thus, Muslims are enjoined to recite the following supplication before entering such places, “O Allaah, I seek refuge in you from the evil male and female jinn.” The jinn find it easiest to enter from the anus so this is the most common entrance. However, they also gain access from other orifices, including the eye. Q. And how do they leave? A. From the same places that they enter. Q. In which part of the human body do the jinn dwell? A. When the jinn enter the human body, they settle in the control center of the body – the brain. The concentrate in the brain and conceal the human mind, making the person lose consciousness in a way similar to hypnotism. Then they manifest themselves and take control of the body through the brain. However, this does not mean that they only concentrate in the brain. They may concentrate in other body parts and organs, thereby leaving the brain. Q. During exorcisms have you ever experienced any attempts by the jinn to possess you? A. I praise Allaah and give thanks to Him in the way appropriate to His glory. My shaykh, Ibn Taymeeyah (may Allaah have mercy upon him) said in his book, al-Fataawaa, “Applying this knowledge of spiritual medicine and/or Qur’ânic medicine is compulsory upon whoever learns it. Because it is equivalent to relieving the troubled, helping the oppressed, liberating the distressed and supporting the weak. It is among the greatest branches of fighting in the path of Allaah (jihaad fee sabeelillaah).” He also said, “Those who work in this field are feared by the jinn because they know that they (i.e., the exorcists) do it as a means of pleasing Allaah. Thus, Allaah places in the soul of the jinnee a fear of the exorcist.” I have never experienced a jinnee attack while I was awake. However, if I go to sleep without making the protective supplications, the jinn hurt me during my sleep and make me restless. Whenever this happens, I awaken quickly and recite the supplications of divine refuge (ta’awwudhaat) and protection, and Allaah protects me. Q. Since you began exorcising people over 40 years ago, have any of your family members been possessed? A. I have not experienced it within my family. However, whenever devils fail in their attack on the human soul, they will try an external attack by setting his family against him, such as his wife, child, mother, father or leader. But such attacks are comparatively mild. If the exorcist has strong faith in Allaah and is truthful and pious, external attacks will also fail. I would like to advise those who wish to work in this field to be careful. On one occasion when I was exorcising a jinnee by the name of Jibreel, who had been severely hurting a woman (and this was around the time I began exorcising), I said to it, “Jibreel, leave the woman and come into my body. Give her a break. Perhaps Allaah will give me more strength and health to bear your presence.” Jibreel was silent for a moment, then he said, “From where will I enter you? From which part can I? I took this as glad tidings from Allaah that He was protecting me by sending angels who would ward off the evil of the jinn. For Allaah has made a type of angel which is specifically for the protection of humans, according to the text of the Qur’aan: “Surely, every soul has a protector over it.”[12] |
Ibn Taymeeyah suggested the following three circumstances to be the main reason why jinn may possess humans: 1. “The occasional possession of man by the jinn may be due to sensual desires on the part of the jinn…or even love, just as it may be among humans 2. “Demonic possession sometimes also occurs as a result of horseplay, jest or plain evil on the part of the jinn, just as evil and mischief occurs among the humans for similar reasons.” 3. “However, possession is most often a result of the jinn being angry because some wrong has been done to them. Thus, the jinn punish those who wronged them. For example, when humans accidentally harm them or hurt them by urinating on them, by pouring hot water on them, or by killing some of them, the jinn think that they have been intentionally harmed. Although humans may not realize what they have done, the jinn are by nature very ignorant, harsh and volatile in their behavior, so they may vengefully punish humans much more severely than they deserve ALLAH KNOWS BEST |
* do they go back to where they came from? It depends, In my experience of witnessing Islamic exorcism the jinns could go back to where they came from promising not to harm any human unless he wants the Wrath of God or become muslims and travel to where other muslim jinns live and dedicate the rest of their lives to the worship of Almighty Allah and not harming anyone ever again. where do they come from? Prophet Muhammad (saw) said: The jinn are of three types: a type that has wings and they fly through the air; a type that looks like snakes and dogs; and a type that stops for a rest then resumes its journey.Some jinns live in Forests,Holes, abandoned building/building in ruins, mountains or Caves.They are mostly to be found in ruins and unclean places like bathrooms, dunghills, garbage dumps and graveyards. Hence the Prophet (peace and blessings be upon him) taught us to take precautions when entering such places, by reciting the adhkar (mentioning Allah’s Name) prescribed by Islam* do they enter the next available body? In Islam the jinn leaving the possessed is made to promise never to possess any other human being unles he wants the Wrath of Almighty Allah to be upon him or her. *Do they wander around the earth looking for a host body to enter? `Jinns dwell on Earth just like we humans,they have families,tribes,animals,religions(Muslims,Christians,Jews,Buddist,Hindu,etc),sects.There were created by God Before the Children of Adam ,they are the same Creation with satan. Most of the time the humans are the ones who invoke the jinns to possess any perceived enemy with black magic through the help of babalawo,dibia,boka etc and they ask for human body parts,animals etc as a ritual sacrifice and worship in return for their services. * or do they automatically cease to exist? Jinns dont die automatically unless his appointed time for Death arises just like human dies,However they have longer Life span than humans they live thousands of years and can have many Children at a time.Hell and Heaven is meant for the dead ,Jinns will either go to heaven or hell when they die depending on what good and evil they did on Earth Before they die.They will be judged by God Almighty on the day of Júdgement the same way we humans will be judged on the Day of Judgement. ALLAH KNOWS BEST |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
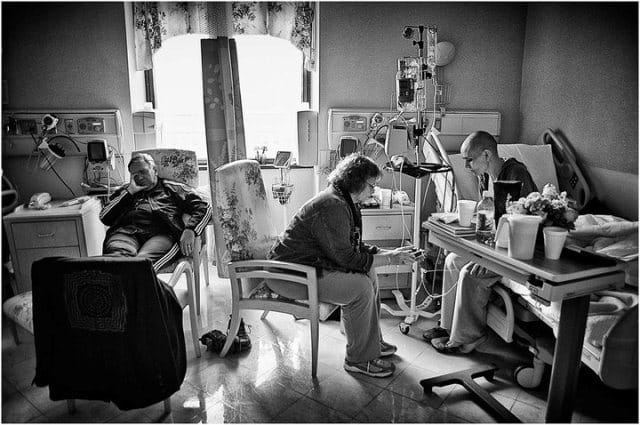{kind=link}
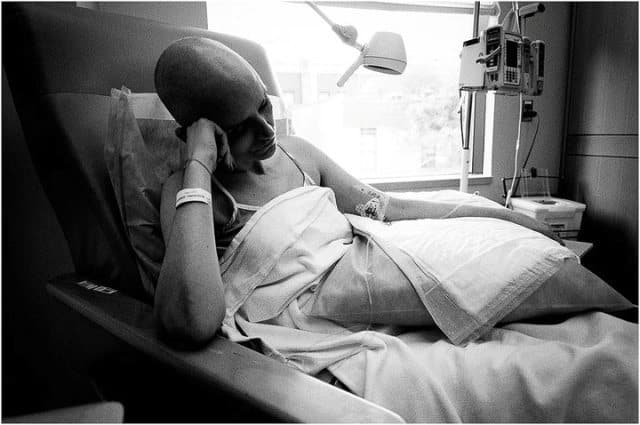{kind=link}
{kind=link}
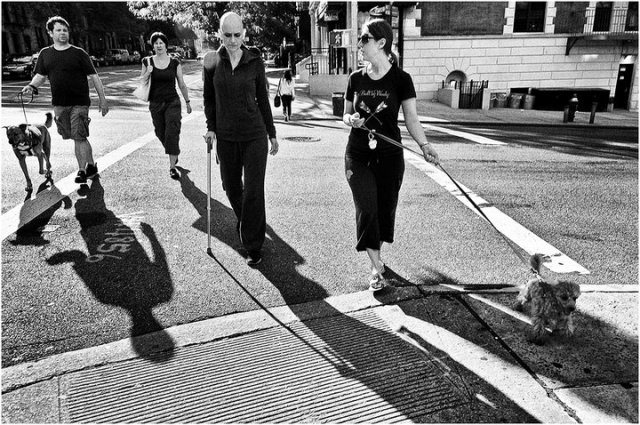{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
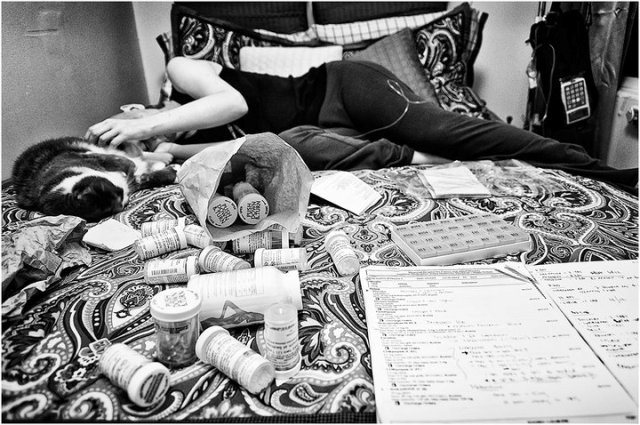{kind=link}
{kind=link}
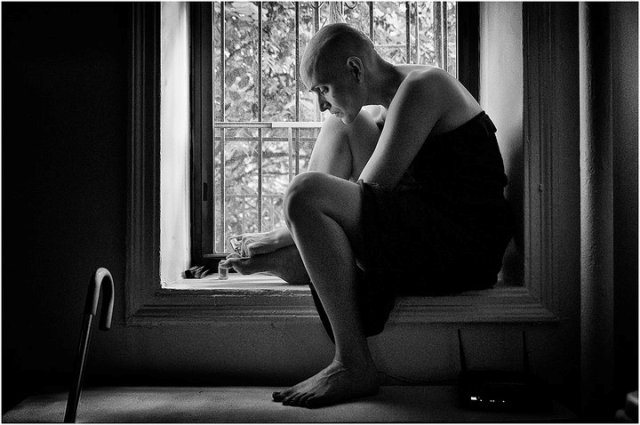{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1 2 3 4 5 6 7 8 ... 27 28 29 30 31 32 33 34 35 (of 44 pages)